Emily Dykstra, Research Manager –
During plan year 2020, CMS established prior authorizations in Medicare Parts A and B for five very specific outpatient department (OPD) services and since has added only three to the list for a total of eight services.1 However, in January 2026, CMS will add an additional 17 services to those requiring prior authorization, piloting it in six states. They will also roll out a pilot program using an Artificial Intelligence (AI)/Machine Learning (ML) model, called WISeR, to execute the expanded prior authorization process.2,3 CMS is positioning this increase to prior authorizations as a way to cut fraud, waste, and abuse. Further, CMS will provide incentives to companies who can lower spending in Medicare parts A and B, particularly those who have already demonstrated competence with using AI and ML in their prior authorization processes, leaving the door open to additional services being added in the future.
Medicare beneficiaries will likely not receive these changes well. As Deft has shown most recently in the 2025 Medicare Age-In Study, in addition to a wide-network system, one of the main reasons seniors choose to keep Medicare A and B only—with or without a Medigap plan—is not having to worry about availability of care, essentially avoiding managed care. Half of age-ins leaning toward Medigap plans named “wanting to be able to use any doctor or hospital” as their top reason for choosing Medigap, with 27% saying they “want coverage that is guaranteed and will not change”, referring to the possibility of a service falling under a prior authorization with an MA plan. Additionally, seniors are often very distrusting of AI in terms of health care/prior authorizations, as seen in Deft’s 2024 Medicare Digital Tools Study where 69% of seniors did not think AI could fairly handle the approval or denial of medical procedures.
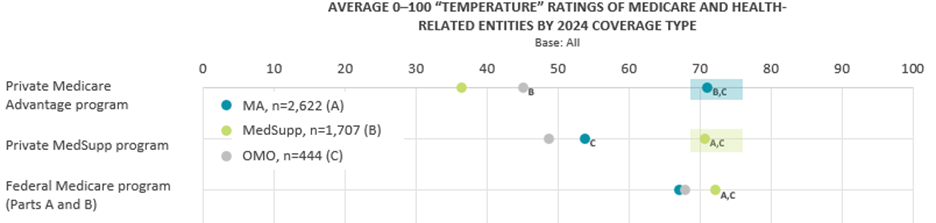
Recent news has focused on the difficulties of prior authorization, with KFF reporting MA insurers made almost 50 million prior authorization determinations in 2023 alone.4 Even though denials were down and 80% of appeals were successful, the prior authorization process is taxing to members and health providers.5 It is unsurprising then that private insurance has remained relatively unpopular among Medicare A and B only and Medigap recipients. As seen in the “Average Temperature Ratings” chart below from Deft’s 2025 Medicare Shopping and Switching Study, traditional Medicare and Medigap beneficiaries gave significantly lower ratings for private Medicare insurance compared to the those in Medicare Advantage plans (36 and 45 vs. 71, respectively); much lower than they gave for either Medicare parts A and B or Medigap coverage.
However, MA carriers have an opportunity to market to this group of holdouts. If MA carriers can focus marketing on what supplemental benefits traditional Medicare beneficiaries would gain with an MA plan and deemphasize their own prior authorizations, they have a chance to convert customers. Especially if carriers highlight how this experimental rollout has the potential to lead to additional services requiring prior authorizations for Medicare A and B in the future. And while Medigap plans cover the additional costs from traditional Medicare, they will also be subject to these new prior authorizations. Agents who typically steer clients away from Medicare Advantage due to their aversion to prior authorizations may want to change their tactic. In the end, seniors may benefit most by being placed in a private Medicare plan.
While the experimental rollout will start with 17 targeted services in just six states, MA carriers have an opportunity to shape the narrative and potentially convert traditionally reticent Medicare A and B recipients. The future of prior authorizations in traditional Medicare is unknown at the present, and the expansion of services and states included in this expansion is definitely not off the table. If fee-for-service Medicare becomes increasingly managed, it might make Medicare Advantage more appealing to those who have been resistant in the past.
Sources